

PMS, Perimenopause, Menopause in Women
Background of my interest
In 1996 after publishing an operative book with Harry Miller Critical Operative Maneuvers In Urologic Surgery by Mosby publishers then and now Harcourt, I started performing more pelvic cancer surgery on females with extensive bladder cancers and other pelvic cancers with a team of surgeons, removing the bladder, uterus, and part of the colon with reconstruction of the urinary tract and reconstruction of the vagina. Many patients were young and I made it my goal to reconstruct the most functional vaginal vault possible as I knew that their lives will be difficult in the time ahead. By use of preoperative estrogens and progestins treatment 1 month before the elective surgery to assure that the vaginal walls and the bladder and pelvis connective and muscular tissues were strong, moist, and elastic, we achieved excellent vaginal reconstruction and I became known for these operations. Many patients came from California and insisted on using “Human identical hormones or bioidentical hormones, Estradiol and Progesterone instead of what I was using, Premarin creams and Provera- and the results were the same!

I had an “awakening moment” when one woman asked me for supply of estradiol cream patch (Vivelle) and Progesterone 200 mg with a Progesterone 20 mg topical for 1 year -WHY
Because this was the first time in 15 years that she was able to sleep!
I realized after talking to her that as a surgeon, my single -minded focus on the reconstruction of pelvic tissues and the cancer surgery had made me oblivious to the powerful effects of these hormones on the rest of the body especially the brain and its GABA receptors.
From that day on, in 2001, I realized that these sex hormones affected the whole body function, top to the bottom, and I needed to learn a lot more about what hormones did to the body
Evolution and Physiology
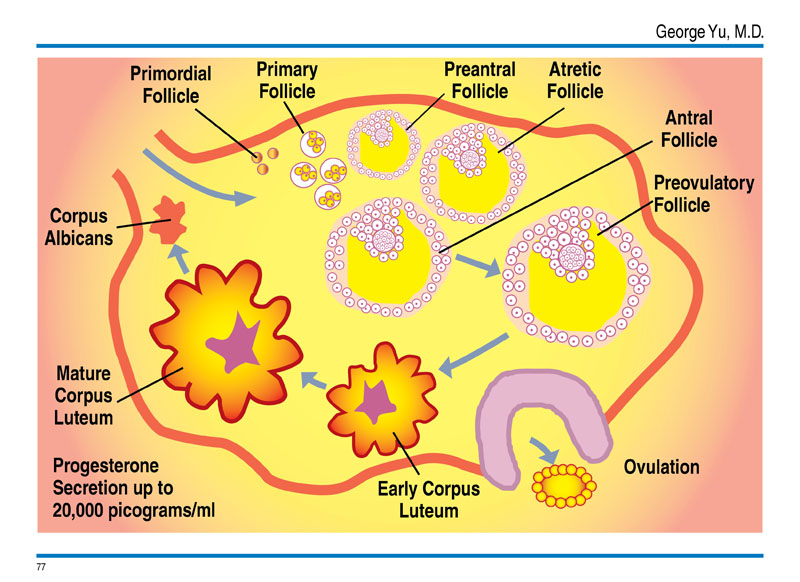
Females are born with about 2 million immature eggs total from her ovaries. In primitive and hunters and gatherers societies, the woman’s ability to procreate offspring was vital for survival of the family and race. When women bore more than 5 to 10 children or more, the monthly menstrual cycles diminishes and pauses until the breast feeding ends and another cycle starts in preparation for future offspring. Therefore her total menstrual history amounts to 20 times at most.
Throughout her life, the vast majority of follicles will die (atresia). Atresia begins at birth and continues throughout the course of the woman's reproductive life. When a woman reaches puberty and starts to menstruate; only about 400,000 follicles remain. With each menstrual cycle, a 1000 follicles are lost and only one lucky little follicle will actually mature into an ovum (egg), which is released into the fallopian tube, kicking off ovulation. Only 1/ 2,000,000 follicles or approximately 400 will ever mature. By age 48, few follicles remain at menopause and unlikely to mature and become viable eggs
In industrialized societies, the modern woman no longer wants or needs to have more than 2 children. But by evolution, women are programed to have another 300 to 400x more menstruations. Therefore she will begin menstruation from age 13 on and finishes with 300 -400 cycles before depleting the supply of follicular eggs and goes into menopause. You might say that our slow evolutionary process of change hasn’t figured that we humans have changing needs and don’t want and don’t need to have so many offspring anymore- and thus the beginning of modern woman’s new problems.
400 Times of Perfect Menstrual Cycles- Impossible?
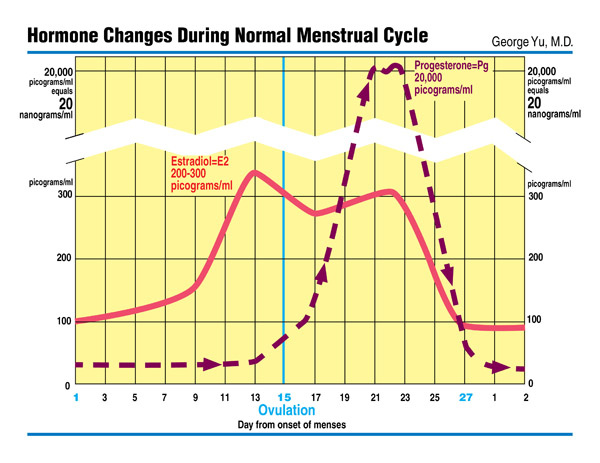
Let alone humans, even machines cannot execute such complicated processes of ovulation with an Estradiol Estrogen rise and a sequential Progesterone rise (100 -200x higher than estrogens) with uterine endometrial preparation for egg implantation perfectly every time! Therefore it is the imperfection of this delicate balance especially these 2 hormones secretions at the right amount and right timing that leads some women to severe symptoms of Premenstrual Syndrome (PMS) and Perimenopause symptoms.
We believe it is the spectrum of imperfection of balancing of these 2 hormones every 400x in a woman’s lifetime which results in the overt symptoms of PMS and Perimenopause with the final end of Menopausal symptoms all from excess or deficiency of Estradiol Estrogens (plus Estriol and Estrone) to the deficiency of Progesterone to counter balance and dominate its partner hormone.
Symptoms, Signs & Findings
Profound symptoms of PMS, symptoms of bloating with breast swelling and tenderness, mood swings, mental dysfunction, craving sweets, and sleep disruptions are indication of Hormone Estrogen Dominance (HED) overriding Progesterone secretions before menstruation. After 400 cycles of menstruation when follicles are depleted, Menopause sets in with a recurrence of “relative” Estrogen Dominance even with Estradiol Estrogen decline as the Progesterone decline is much more pronounced-This change leads to a host of future body changes and cancers
Though some women are blessed with fewer symptoms such as “Hot Flashes” in their passage, by blood testing of the pituitary hormones and sex hormones we can confirm that Menopause is ongoing and relentless with short and long term consequences in the immediate future.
In Menopause, more devastating than “hot flashes”, are sleep fragmentation and deprivations which will be for the lifetime ahead. This is the most common symptom we see in the clinic. Recent research also point to increasing sleep apnea in women at this age period. The weight gain (despite active lifestyle),
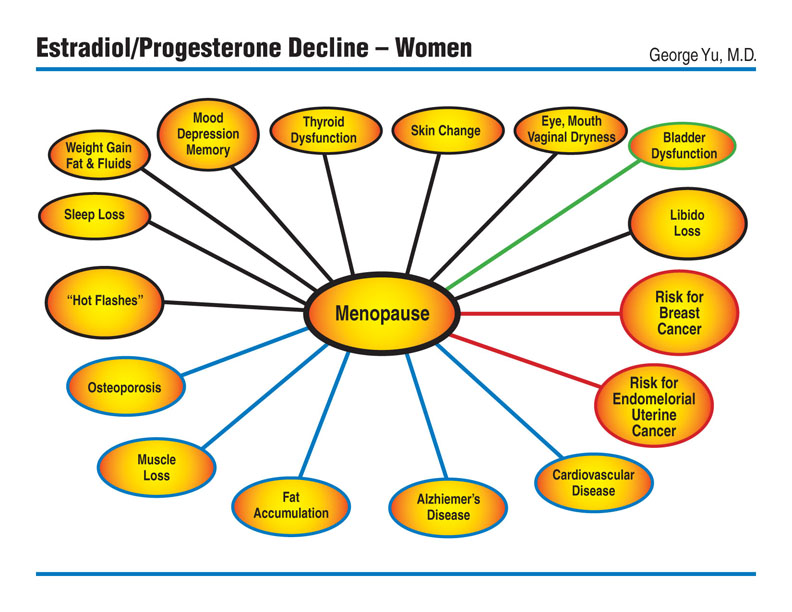
mood fluctuations from happy to depression, the changes in the mucous membranes in dry eyes, dry mouth, and dry vaginal walls (uncomfortable dryness during intercourse), loss of libido, with memory inefficiencies (unable to multi-task a female characteristic) are the more obvious signs and symptoms of the menopause. The obvious skin wrinkles and spots appear despite “Plastic surgery”, mild urinary stress incontinence and over-active bladders, the loss of muscle mass changing the “The Shape of Your Weight” (sacropenia) and osteoporosis are all manifestations which persist and progress as all signaling hormones of progesterone, estradiol, testosterone, DHEA, and growth hormone shifts your whole body from an Anabolic phase (growth and repair state) to Catabolic phase (atrophy and breakdown with default tissue fat- a form of stem cells).
Further, Estradiol Estrogen dominance over progesterone can lead to uterine fibroids, dense and fibrocystic breast on mammography and to thyroid dysfunctions in the form of subclinical and clinical “Hypothyroidism”.
“Dense breasts” on mammography is an indication of Estradiol Estrogen dominance stimulating residual glandular tissues putting women at future risk for cancer but this can be avoided as shown on the photos. Higher Estradiol Estrogen levels puts women at higher risk for uterine cancers especially those who never had children.
Lifestyle and diet effect and exacerbate menopausal symptoms and body changes. Those who are heavy sugar consumers and alcoholic beverages will have more pronounced symptoms. On PET scans looking at sugar intake of cells, breast cancers are known to have high sugar content within the cancer cells.
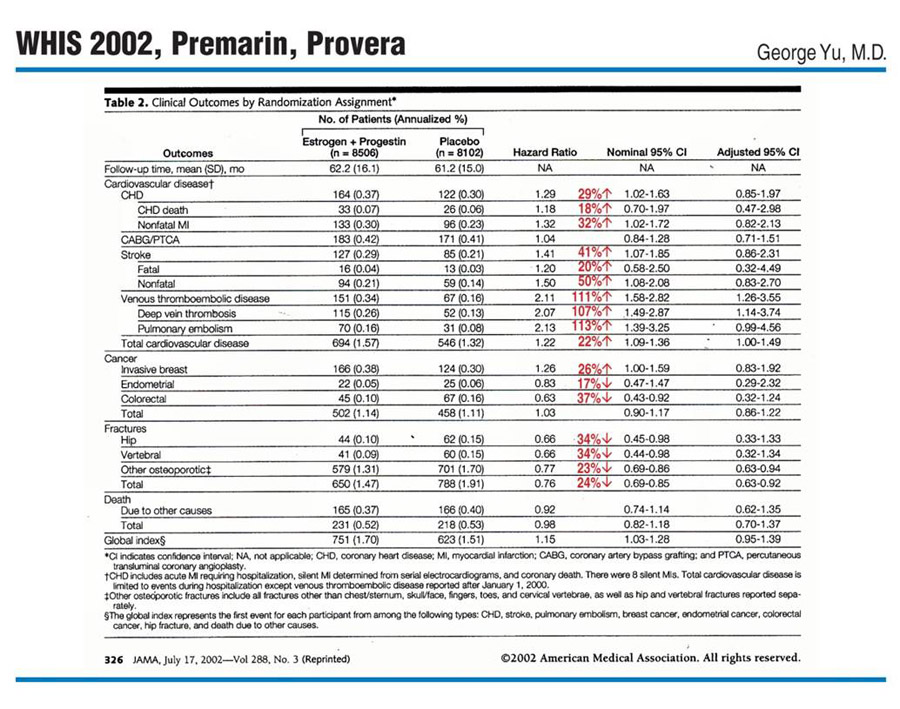
The Best Study in the World & Why Doctors Don’t Like Hormones
Ever since the Women's Health Initiative Study of 2002, most doctors do not prescribe any kind of sex hormone replacements. We as doctors make the assumption that all hormones whether, Premarin equine horse estrogen hormones (CEE) or synthetic progesterone (Provera) are the same as "human identical" sex hormones.
Our body especially the liver recognizes every little change in the steroid structure -testosterone, estradiol, progesterone, cortisol, aldosterone, DHEA adrenal hormone and even Vitamin D (misnomer as it is also a steroid hormone) all look similar with minimal structural changes from the parent molecule Cholesterol.
Man -made hormones are a slight change or an “Analogue “classified as SERM and SARM which mimic the real God- given hormones and the body recognizes the difference. The reason we make synthetic hormones is that the liver cannot metabolize as quickly and therefore the drug is active longer! Another incentive to make “look-alike hormones” or analogues is that you can patent it whereas God made hormones cannot be patented- you can understand why a for-profit company must be able to patent drugs. (Bibliography in reference sections)
Our Smart Liver Knows Everything
The liver, our powerful metabolizing and detoxification organ, or as Dr. Jonathan Wright put it “Our Body Custom House” recognizes every molecule and every steroid hormone and small changes will result in the liver making new protein secretion which later lead to adverse factors in health. At the beginning of Women’s Liberation in the 1950s and 60s the propagation of Birth Control Pills (BCP) had a major social impact but the higher concentrations of the synthetic BC used then lead to liver proteins production leading to “leg blood clots”, thrombosis and to pulmonary embolus as a major complication. Today doses are smaller and combinations are fine-tuned but the liver still recognizes the synthetic hormones! In the past we used Diethylstilbestrol (DES) another synthetic hormone on men with advanced prostate cancers and in the Netherlands where male to female sex changes used synthetic estrogens and progesterone, both of which led to higher risks for venous blood clots (thrombosis) with the complications of pulmonary embolus.
I highly recommend all of you to read an profound and informative article in Vanity Fair January 2014 issue titled “Danger in the Ring” by Marie Brenner revealing the complications so many women have suffered with venous leg clots (thrombosis) and more severe complications of pulmonary embolus and death among Nuvaring contraceptive containing another SERM progestin, Desogestrel. This article will give you the history of the FDA, the industry, and the litigations involved with many other birth control hormones used today. The more detailed analysis of the dangers of the Nuvaring is in the scholarly research by O Lidegaard of Denmark in British Medical Journal May 2009 and 2012 Venous thrombosis in users of non-oral hormonal contraception: follow-up study, Denmark 2001-2010.
This is the same experience I witnessed as a surgical resident in 1976 when a young woman died from a massive pulmonary embolus when the birth control pills with higher dose of hormones. Today the industry has learned to titrate the doses down and using different combination of synthetic estrogens and synthetic progestins to avoid overt clinical problems seen in the past, but the liver still recognizes these synthetic hormones and continues to make proteins which can make your blood more “Clots” prone.
When will we learn that synthetic hormones are not good and human identical hormones in proper balance are what God and evolution has designed for our complex female body?
Our Philosophy on Female Hormone Replacement
“Mimic Nature But Never Let Nature Know What You Are Doing”
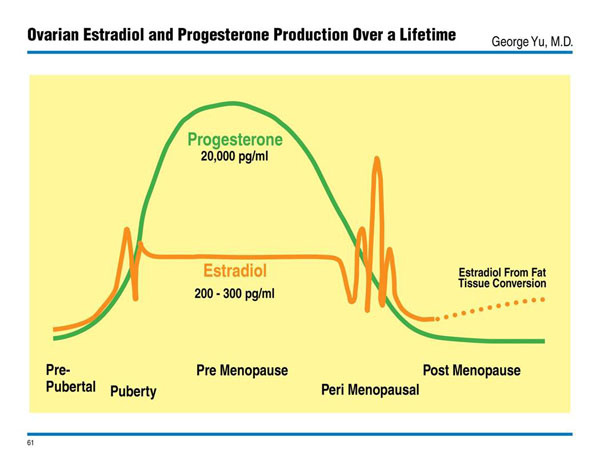
The best phase of womanhood is between 20 to mid-30s show the highest ratio of Progesterone / Estradiol Estrogens of approximately 100-200 / 1. We believe a relative proximate ratio of Progesterone dominance over Estradiol Estrogen will keep the woman healthy and beautiful. (Bibliography in reference sections)
Testing Who You Are “Snapshot of your Hormone Movie”
You have choices of venous blood testing, finger blood spot testing, urine testing and sometimes saliva testing. the pituitary hormones LH and FSH, sex hormones Estradiol, Estriol, Estrone, Progesterone, Testosterone and SHBG with thyroid TSH, Free T4, Free T3, adrenal hormone DHEA and Cortisol and pancreatic Insulin and Hemoglobin A1c are an important baseline.
“One Shoe Does Not Fit All”- adjusting, cycling, and finding the right combination of hormone replacement
My experience of 30 years from past surgical career and the present experience have shown me that each woman is different from the other and genetic polymorphism require tailor- made regimen for each person despite overall bell curve normal ranges established from clinical studies and laboratory samplings.
Simultaneously, we begin a slow process of “Mimic Nature without letting Nature know” what we are doing with replacing a human identical estrogens, progesterone and testosterone, thyroid etc. and cycling off and on subtly.